If you code, review, or bill for home health assessments, 2025 brought a new version of the assessment instrument you build every episode around. On January 1, 2025, the Centers for Medicare & Medicaid Services (CMS) replaced OASIS-E with OASIS-E1. Compared with the sweeping OASIS-E overhaul of 2023, OASIS-E1 is a deliberately small, targeted update: one new item, two retired items, and a handful of clarifications. But "small" is not the same as "ignore it." Anything that changes what your clinicians answer at the point of care ripples straight into your case-mix, your Quality Reporting Program (QRP) compliance, and ultimately your cash.
This guide walks through exactly what changed from OASIS-E to OASIS-E1, when it took effect, and — most importantly for revenue teams — how those changes touch coding, quality reporting, and billing. Every item-level change below is tied to CMS's official OASIS-E1 data set and the CY 2025 Home Health Prospective Payment System (HH PPS) Final Rule so you can verify it against the primary source.
What Is OASIS-E1, and Why Did CMS Release It?
The Outcome and Assessment Information Set (OASIS) is the standardized patient assessment that Medicare-certified home health agencies (HHAs) complete at defined time points — Start of Care (SOC), Resumption of Care (ROC), recertification, other follow-up, Transfer, Discharge, and Death at Home. OASIS data feeds three separate machines at once: the Patient-Driven Groupings Model (PDGM) that sets your payment, the HH QRP that measures quality, and the expanded Home Health Value-Based Purchasing (HHVBP) model.
OASIS-E1 is a point revision of OASIS-E rather than a ground-up redesign. CMS posted the final OASIS-E1 instrument and guidance manual with an effective date of January 1, 2025, published on the agency's OASIS Data Sets page alongside the OASIS-E1 All-Items instrument. The driving reason for the update was to operationalize a quality measure that had already been finalized in an earlier rule: the COVID-19 vaccine measure. To make room for it and to clean up items CMS no longer uses, the agency added one item, removed two, and refined instructions on several others.
The practical takeaway: any assessment with a Start of Care date, or a time point occurring, on or after January 1, 2025 must use OASIS-E1. Assessments already in progress under OASIS-E followed the prior instrument based on their time point dates, but from the new year forward the E1 version is the only compliant instrument.
What Changed From OASIS-E to OASIS-E1
Here is the short version, verified against CMS's OASIS-E1 instrument and change documentation. Below the summary, each change is explained in plain language.
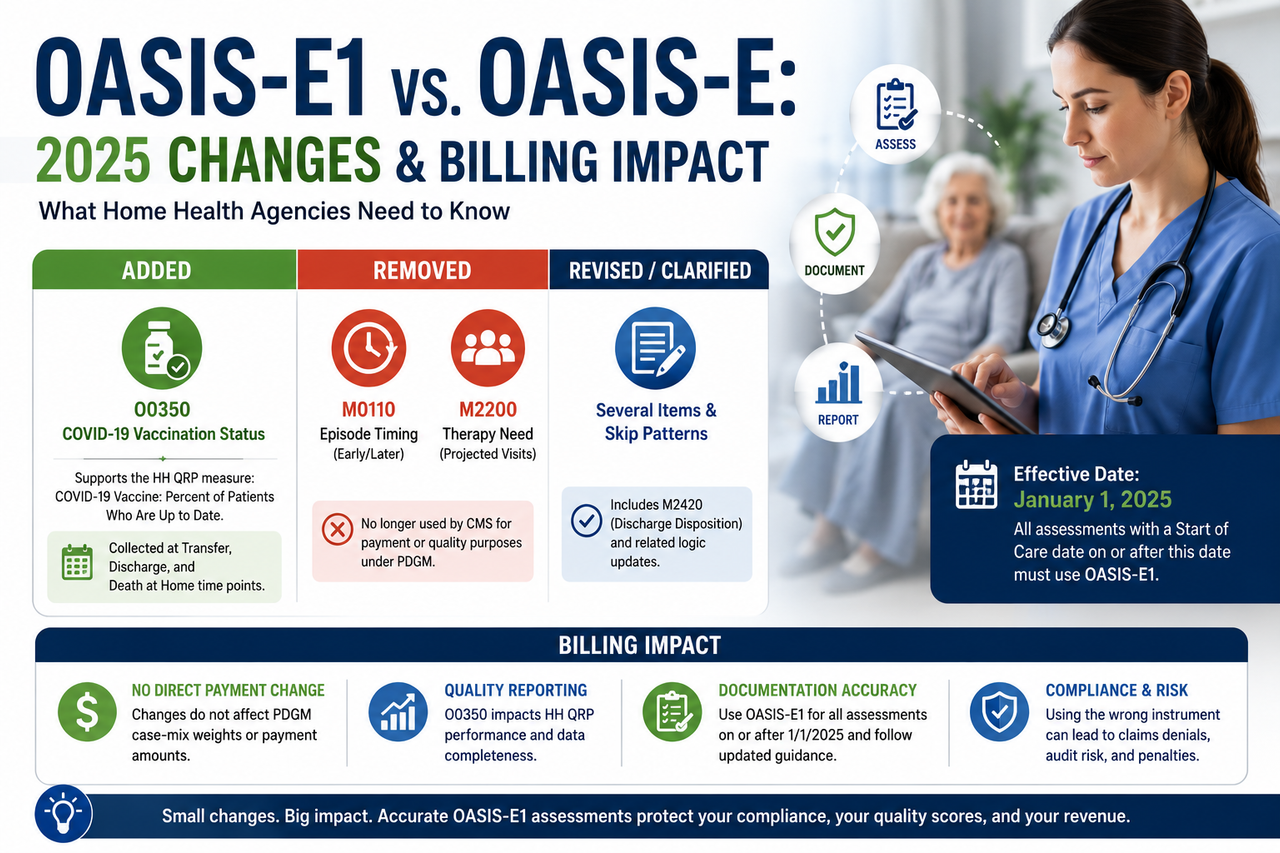
- Added: One new item — O0350, the patient's COVID-19 vaccination status.
- Removed: Two items no longer used by CMS — M0110 (Episode Timing) and M2200 (Therapy Need).
- Revised: Clarifications and skip-pattern adjustments to a handful of existing items, including M2420 (Discharge Disposition) and related logic tied to the removed items.
The New Item: O0350, COVID-19 Vaccination Status
The single new item in OASIS-E1 is O0350 — Patient's COVID-19 vaccination is up to date. It supports the "COVID-19 Vaccine: Percent of Patients/Residents Who Are Up to Date" quality measure, which CMS finalized in the CY 2024 HH PPS Final Rule (CMS-1780-F) for adoption beginning with the CY 2025 HH QRP. In other words, the measure was written into policy in 2023; OASIS-E1 is simply the instrument that finally carries the data element to collect it.
Per CMS's OASIS-E1 instrument, O0350 is collected at the Transfer, Discharge, and Death at Home time points rather than at Start of Care. It asks, in effect, whether the patient's COVID-19 vaccination status is up to date according to current Centers for Disease Control and Prevention (CDC) guidance at the time of assessment. Because "up to date" is defined by CDC recommendations that evolve, agencies should follow the response guidance in the current OASIS-E1 guidance manual and CDC criteria in effect on the assessment date rather than a fixed dose count.
For revenue and compliance teams the key point is where this item lives in the payment-versus-quality split: O0350 is a QRP measure item, not a PDGM case-mix item. It does not change the HIPPS code or the payment amount for the period. It does, however, count toward your QRP data-completeness obligations, which we cover in the billing section below.
The Removed Items: M0110 (Episode Timing) and M2200 (Therapy Need)
OASIS-E1 removes two legacy items that CMS no longer uses for the HH QRP or other agency purposes:
- M0110 — Episode Timing (whether the payment episode was "early" or "later"). This concept mattered under the old 60-day, therapy-threshold payment system. Under PDGM, timing is derived by CMS from claims data — specifically, whether a 30-day period is the first ("early") or a subsequent ("late") period in a sequence — so the clinician-reported OASIS item became redundant.
- M2200 — Therapy Need (the projected number of therapy visits). This item drove payment in the pre-2020 model, where therapy volume directly influenced reimbursement. PDGM eliminated therapy thresholds as a payment factor, leaving M2200 with no payment or quality role.
Removing these items is a housekeeping move: CMS is retiring data it stopped using when PDGM took effect in 2020. Because both items had already been severed from payment logic, their removal does not by itself change what any 30-day period pays. Removal did, however, require CMS to adjust the surrounding skip patterns and item flow — for example, logic that previously routed around M0110 at SOC and ROC. Agencies should confirm their EHR/OASIS software vendor updated the instrument flow so clinicians are not prompted for retired items and are routed correctly through the remaining SOC/ROC questions. When in doubt about exact skip-pattern wording, defer to the current OASIS-E1 All-Items instrument.
Revised Items and Clarifications
Beyond the one addition and two removals, OASIS-E1 refines guidance on several existing items rather than changing their scoring intent. The most frequently cited example is M2420 (Discharge Disposition), where CMS clarified the response language around the type of ongoing formal services a discharged patient is transferred to. Other clarifications touch item instructions and interview guidance elsewhere in the instrument.
Because these are wording and instruction refinements rather than new scoring rules, the safest approach is to read the change descriptions in the official OASIS-E1 guidance manual before retraining staff, rather than relying on secondary summaries. CMS maintains the authoritative change documentation and manual on its OASIS Data Sets page, and posts implementation notes on the Home Health QRP Spotlight and Announcements page. If a specific item's revised wording affects how your clinicians answer it, treat the manual — not a blog, including this one — as the source of truth.
The Effective Date and the All-Payer OASIS Transition
Two 2025 changes are easy to conflate but are legally distinct. Keep them separate:
1. OASIS-E1 instrument effective date: January 1, 2025. This is a change to *which version* of the assessment you complete. 2. All-payer OASIS collection: a change to *which patients* you must assess, phased in during 2025.
Historically, the OASIS requirement centered on Medicare and Medicaid patients. Under the phased all-payer expansion, CMS made OASIS collection and submission voluntary for non-Medicare/non-Medicaid patients from January 1 through June 30, 2025, then mandatory for patients of any pay source (who are not otherwise exempt) beginning July 1, 2025. CMS documented this timeline in its Home Health OASIS All-Payer Q&As and on the Home Health Quality Reporting Requirements page.
The existing exemptions did not change: patients under 18, patients receiving maternity services, and patients receiving only personal care, homemaker, or chore services remain outside the OASIS requirement. The combined effect is that from July 1, 2025 forward, most agencies are completing OASIS-E1 on a substantially larger share of their census than before — which is precisely why assessment accuracy and coding throughput became a bigger operational lever in 2025.
Why OASIS-E1 Matters for Coding, Quality, and Billing
This is where a "minor" instrument update earns real attention. OASIS is not paperwork that sits beside the claim — it *is* the claim's engine. Three distinct financial pathways run through it.
Impact on PDGM Case-Mix and the HIPPS Code
Under PDGM, each 30-day period is assigned to a case-mix group built from admission source, period timing, clinical grouping (driven by the principal diagnosis), functional impairment level (driven by specific OASIS GG-series and related items), and a comorbidity adjustment (driven by secondary diagnoses). Those inputs generate the HIPPS code on the claim, which sets the payment. The CY 2025 HH PPS Final Rule (CMS-1803-F) preserved this structure.
Here's the good news about OASIS-E1 specifically: the two removed items (M0110 and M2200) were not PDGM case-mix inputs, and the new item (O0350) is a QRP item, not a case-mix input. So OASIS-E1 does not, by itself, re-weight any payment group. The functional and diagnosis items that actually drive your HIPPS code are unchanged in intent. What changes is the surrounding discipline: with all-payer collection expanding volume and CMS refining item instructions, the cost of a *sloppy* functional or diagnosis assessment is now spread across more episodes. Accurate scoring on the payment-driving items remains the single largest OASIS lever on revenue, which is why a disciplined coding and OASIS review process pays for itself.
Impact on the HH QRP and the 2% Payment Penalty
The COVID-19 vaccine item is the part of OASIS-E1 with the most direct compliance teeth. HH QRP measures like this one carry a data-completeness requirement, and agencies that fail to meet the QRP reporting threshold face a reduction of the annual payment update by two percentage points. That penalty applies to your entire Medicare payment update for the year — a far larger dollar figure than any single claim.
Because O0350 is collected only at Transfer, Discharge, and Death at Home, the risk is a quiet one: clinicians focused on SOC accuracy may under-attend to end-of-episode items, leaving blanks or "unknown" responses that erode your completeness percentage over a full year. Building the vaccine item into discharge workflows and auditing it in your clinical documentation review is the cheapest insurance against a QRP penalty that dwarfs the effort of collecting it.
Impact on Billing Operations and Cash Flow
Even without changing case-mix weights, OASIS-E1 touches billing operations in three concrete ways:
- Software readiness. Retired items and adjusted skip patterns mean your EHR must be on the correct instrument version. A vendor that lags on the update can produce assessments that reject at the state submission system, delaying the Request for Anticipated Payment/period claim that depends on a locked, accepted OASIS.
- Larger assessed population. All-payer collection means OASIS completion is now a gating step for more patients. Bottlenecks in assessment review and coding directly delay claim submission and lengthen days in accounts receivable.
- Clean-claim dependency. The HIPPS code on the claim must match the finalized OASIS. Any mismatch between the assessment and the coded diagnoses is a denial waiting to happen. Tightening the handoff from clinician to coder to biller is core revenue cycle management work, and it is where OASIS-E1's operational load actually lands.
The 2025 Payment Backdrop You Should Read Alongside OASIS-E1
OASIS-E1 arrived at the same time as the CY 2025 payment update, and it helps to see them together. In the CY 2025 HH PPS Final Rule (CMS-1803-F), published in the Federal Register on November 7, 2024, CMS estimated that aggregate Medicare payments to HHAs in CY 2025 would increase by 0.5%, or about $85 million, relative to CY 2024.
That modest net number is a blend of moving parts: a home health payment update of roughly 2.7%, partially offset by a permanent behavioral adjustment of -1.975% (half of the full calculated adjustment) tied to PDGM behavior assumptions, plus a small offset from an updated fixed-dollar loss ratio for outlier payments. The lesson for revenue teams is blunt: with the net update near flat and behavioral cuts continuing, you cannot count on rate increases to grow revenue. Margin now comes from assessment accuracy, clean coding, and denial prevention — exactly the levers OASIS-E1 puts back in focus.
What Home Health Agencies Should Do Now
If your agency has not already closed the loop on OASIS-E1, treat this as a short, high-leverage checklist:
- Confirm your instrument version. Verify your EHR is on OASIS-E1 for every SOC dated January 1, 2025 or later, and that retired items (M0110, M2200) no longer appear while skip patterns route correctly.
- Operationalize O0350. Add the COVID-19 vaccine item to Transfer, Discharge, and Death at Home workflows, train clinicians to apply current CDC "up to date" criteria, and monitor completeness so it never drags your QRP threshold.
- Extend assessment capacity for all-payer volume. With OASIS mandatory across pay sources since July 1, 2025, make sure your review and coding pipeline scales to the larger census without lengthening days in A/R.
- Retrain on revised items using the manual. Update competencies for M2420 and other clarified items directly from the official OASIS-E1 guidance manual, not secondhand summaries.
- Audit the OASIS-to-claim handoff. Reconcile the finalized assessment against the coded diagnoses and HIPPS code before billing to prevent denials.
- Verify against primary sources. Bookmark CMS's OASIS Data Sets page and QRP Spotlight and Announcements so your policies track the current instrument and guidance.
Handled well, OASIS-E1 is a light lift. Handled carelessly, it becomes a slow leak — a QRP penalty here, a rejected assessment there, a denied claim from a diagnosis mismatch. The agencies that come out ahead treat the assessment as the financial document it truly is and build accuracy in at the point of care.
Frequently Asked Questions
When did OASIS-E1 take effect?
OASIS-E1 became effective on January 1, 2025. Any Start of Care assessment dated January 1, 2025 or later, and any subsequent time point occurring on or after that date, must use the OASIS-E1 instrument. CMS posted the final instrument and guidance manual on its OASIS Data Sets page.
What is the difference between OASIS-E and OASIS-E1?
OASIS-E1 is a targeted revision of OASIS-E, not a full redesign. The core changes are the addition of one item (O0350, COVID-19 vaccination status), the removal of two items CMS no longer uses (M0110 Episode Timing and M2200 Therapy Need), and clarifications to instructions and skip patterns on several existing items such as M2420. You can compare versions directly using the OASIS-E1 All-Items instrument.
What items were removed in OASIS 2025?
CMS removed M0110 (Episode Timing) and M2200 (Therapy Need) in OASIS-E1. Both were legacy items tied to the pre-PDGM payment system and were no longer used by CMS for the HH QRP or payment. Because they were already disconnected from PDGM case-mix, their removal does not change what a 30-day period pays.
What is O0350 in OASIS-E1?
O0350 is the new OASIS-E1 item that records whether the patient's COVID-19 vaccination is up to date, based on current CDC guidance. It supports the COVID-19 vaccine quality measure finalized in the CY 2024 HH PPS Final Rule (CMS-1780-F) and is collected at the Transfer, Discharge, and Death at Home time points.
Does O0350 affect my PDGM payment?
No. O0350 is a Quality Reporting Program (QRP) item, not a PDGM case-mix input, so it does not change your HIPPS code or the payment for a period. It does count toward your QRP data-completeness obligation, and failing to meet the QRP reporting threshold can reduce your annual payment update by two percentage points.
Did OASIS-E1 change how home health claims are paid?
Not directly. The items OASIS-E1 removed (M0110, M2200) were not PDGM case-mix factors, and the item it added (O0350) is a quality measure. Payment continues to flow from admission source, period timing, clinical grouping, functional impairment, and comorbidity adjustment, as preserved in the CY 2025 HH PPS Final Rule (CMS-1803-F). What changed is the operational discipline around assessment accuracy, not the payment formula itself.
What is the all-payer OASIS requirement, and how does it relate to OASIS-E1?
The all-payer expansion is a separate 2025 change to *which patients* require OASIS. CMS made collection voluntary for non-Medicare/non-Medicaid patients from January 1 through June 30, 2025, then mandatory for patients of any (non-exempt) pay source beginning July 1, 2025, per its Home Health OASIS All-Payer Q&As. It is distinct from the OASIS-E1 instrument change but took effect in the same year, so agencies are now completing OASIS-E1 on a larger share of their census.
What was the CY 2025 home health payment update?
CMS estimated aggregate Medicare payments to home health agencies would rise by about 0.5%, or roughly $85 million, in CY 2025. That net figure reflects an approximately 2.7% payment update offset by a permanent behavioral adjustment of -1.975% and a small outlier-related offset, as described in the CY 2025 HH PPS Final Rule fact sheet and the Federal Register notice.
Where can I verify the official OASIS-E1 changes?
Always confirm item-level details against CMS primary sources: the OASIS Data Sets page for the instrument and guidance manual, the OASIS-E1 All-Items PDF for exact item wording and skip patterns, and the Home Health QRP Spotlight and Announcements page for implementation updates. For scoring questions specific to your patients, the guidance manual is the authoritative source.
How can Medeoan help our agency stay compliant and paid accurately?
Medeoan supports home health agencies across the full assessment-to-cash pathway: accurate coding and OASIS review to protect your case-mix, clinical documentation review to keep QRP items like O0350 complete and defensible, and end-to-end revenue cycle management to tighten the OASIS-to-claim handoff and prevent denials. The goal is simple: make sure every accurate assessment turns into a clean, timely, fully paid claim.